
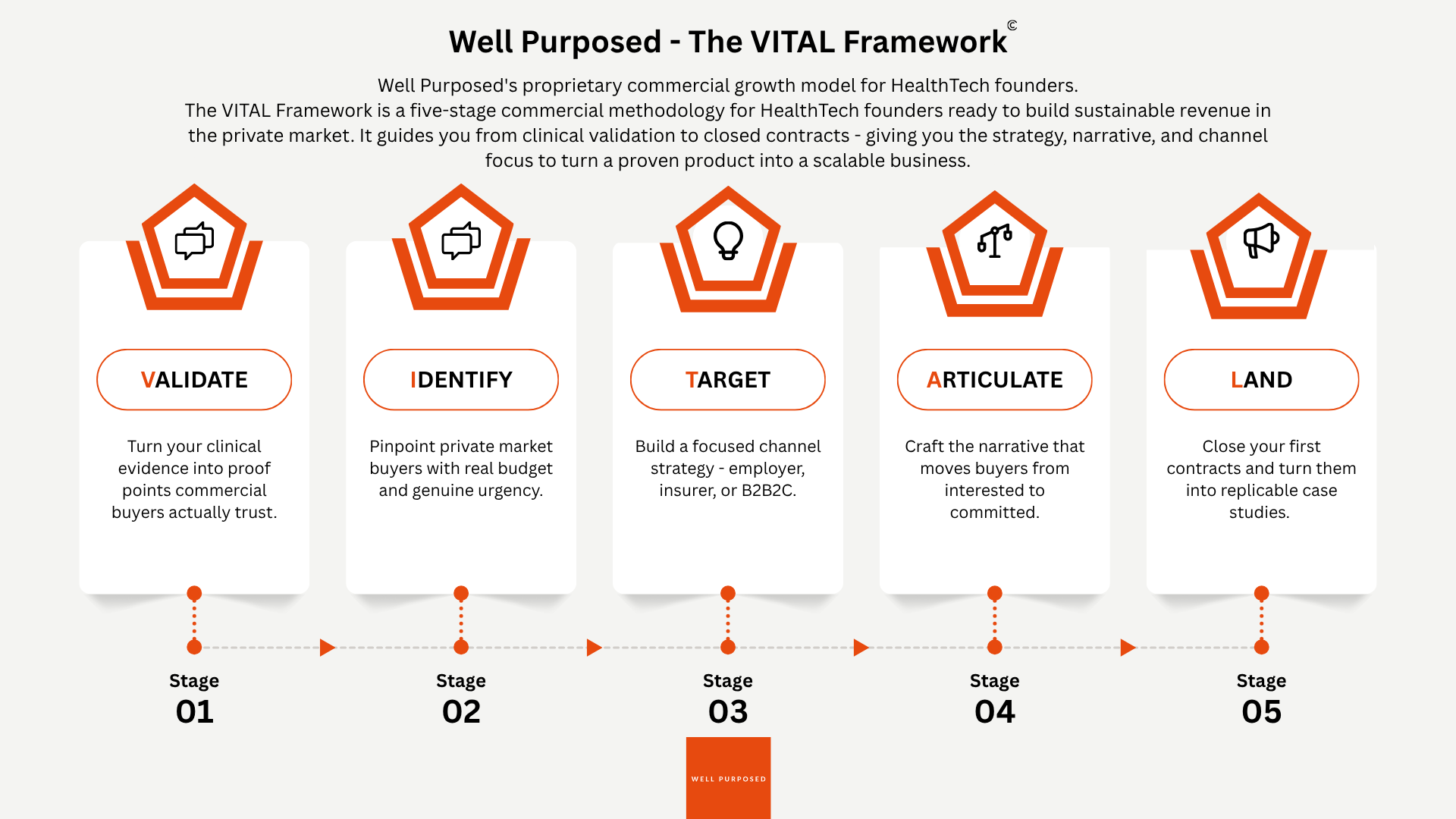
This is the full version of the LinkedIn series introduced over the last five weeks. The series ran one stage per Monday: Validate, Identify, Target, Articulate, Land.
The VITAL Framework is what I use with the Series A HealthTech founders I advise through Well Purposed. It is the operational core of the £3,500 Diagnostic and the structural spine of the Q3 advisory cohort that opens on Monday 8 June.
The gap between "clinical evidence is impressive" and "the commercial conversation closes" is what VITAL is built to navigate. The five stages, in order, that the founders who close consistently have worked through.
Stage 1 - VALIDATE: turn clinical evidence into commercial proof
The first stage is the one most founders think they have already finished, yet haven't.
Clinical validation is the floor. Commercial validation is a different thing. The peer-reviewed paper, the NICE endorsement, the RCT data, all of it matters to clinical buyers, and almost none of it lands with corporate procurement, HR Directors, insurers, or platform partners.
Commercial proof requires translating clinical outcomes into the language the buyer can defend to their CFO in 60 seconds.
What that looks like in practice:
Cost-avoidance models with named assumptions, in a single page the buyer can take into their next meeting.
Sickness-absence comparators (for HR buyers) or claims-data implications (for insurers), drawn from the closest dataset you can reference.
One specific failure mode you pre-empt before the buyer raises it, because the buyer's analyst will raise it whether you do or not.
The founders who close consistently do not have stronger clinical evidence than the founders who stall. They have done the translation work.
Case study. A Series A cardiovascular HealthTech founder I worked with had a strong dataset on a clinical outcome metric but could not close corporate wellness buyers. The breakthrough was rewriting the same evidence as a sickness-absence comparator. Same data. Different audience. Three deals in the next 12 weeks.
Validate means validate the commercial proof points. Your science is already validated. The work is the translation.
Stage 2 - IDENTIFY: stop selling to the market, start selling to a person
The second stage is where most founders confuse aspiration with strategy.
"We sell to employers, insurers, and health-conscious consumers" is not a target market. It is a direction of travel.
Identifying your buyer means naming them at a granular level: job title, seniority, the trigger event that creates urgency this quarter, the budget line they have access to, and the internal politics they are navigating.
Three diagnostic questions to run on your own current pipeline:
Can you name three specific job titles your product is built for, and the size of organisation in which each title has meaningful budget?
Can you describe the trigger event that makes this buyer prioritise your category over six other things on their plate this quarter? Examples: benefits renewal cycle, board mandate on sickness absence, post-restructure people-cost review.
Do you know who in the buyer's organisation is the economic buyer versus the champion versus the blocker, and what each of them needs to feel confident saying yes?
If any of those questions makes you pause, your IDENTIFY work is incomplete. The pipeline volume problem you think you have is actually a buyer-clarity problem. Volume cannot fix it.
Case study. An early-stage women's health platform I advised through the Diagnostic was running a pipeline of 280 corporate prospects. We cut to a named fifty by adding three filters: organisations with active wellbeing budgets not committed for the calendar year, HR Directors with public commitments to women's health programmes, and a recent (within 90 days) trigger event. The closed-deal rate went from 1.2% to 11% on the next thirty conversations.
You do not have a pipeline volume problem. You have a buyer-clarity problem. The two look identical until you have done the IDENTIFY work.
Stage 3 - TARGET: pick one channel and go deep
The third stage is where ambition becomes the enemy of execution.
Having three go-to-market channels in parallel is not ambitious. It is a distraction. The founder with a team of four trying to sell direct to corporates, build a white-label partnership with an insurer, and launch a D2C consumer subscription is achieving activity in all three channels and scale in none.
Each channel is a full-time commercial strategy:
Employer direct. 4–12 week sales cycle. £15k–£150k contract values. HR / People buyer.
Insurer embedded. 6–18 month cycle. Scale-deployment plays. Claims-data and population-health buyer logic.
B2B2C platform. Engagement-metric buyer. Sticky-integration architecture. NPS as the buyer-side success measure.
The founders who scale fastest commit to one channel, win there long enough to produce a reference client and a repeatable commercial model, and only then approach the next channel, with credibility this time.
Channel-selection criteria:
Which channel has the shortest path between your current evidence base and the buyer's purchasing trigger?
Which channel has the highest-value reference clients available to a founder at your stage?
Which channel does your team currently have the relationships to execute against without external hiring?
Case study. A digital therapeutics founder I worked with through the cohort had been hedging across all three channels for 18 months. We picked employer-direct (shortest evidence-to-purchase path), built a focused outreach motion against fifty named accounts, and landed the first three contracts in 11 weeks. The insurer-embedded channel opened twelve months later, but only after the employer-direct case studies existed to anchor the conversation.
Focus is not a limitation on ambition. It is the only architecture that turns ambition into compounding revenue.
Stage 4 - ARTICULATE: the narrative that moves buyers from interested to committed
The fourth stage is the one most founders have built backwards.
The pitch that converts is not the pitch that explains the product better, but one that gives the buyer the language they need to sell the decision internally.
The buyer in the room is not the buyer who signs the contract. The buyer in the room takes your narrative back to their CFO, their board, or their head of procurement; conversations where you are not present. Your job is to give them the exact language, evidence, and counter-arguments they need to win the internal conversation without you.
The narrative that converts answers three questions, pre-emptively, in the order the buyer's analyst will ask them:
Why is this a problem worth solving now - not in the next budget cycle?
Why is your solution the right answer, given everything else they could spend that budget on?
Why should they trust you, specifically, to deliver it?
If your deck doesn't answer all three by slide ten, it is doing the educating job rather than the converting job.
Case study. A HealthTech founder I worked with had a clinically brilliant product and a beautifully designed deck that explained the science in five different ways. We rebuilt the deck around the three-question structure. The next three commercial conversations closed 38% quicker.
Buyers move when they feel understood, not when they feel impressed. The narrative is not for the buyer in the room, it is for the conversation the buyer has after they leave your meeting.
Stage 5 - LAND: design the first contract as infrastructure
The fifth and final stage is where most HealthTech founders leave the most value on the table.
The first contract is not just revenue. It is the marketing asset every subsequent deal will be built on. A real client, in a real organisation, with real outcomes data, willing to be named as a reference, that is worth more to your commercial momentum than any thought leadership, any award, any conference.
But it only becomes that asset if you design it that way from the start.
Four operational moves to build into your first commercial contract:
Price to close, not to maximise margin. The commercial return comes later. Right now, you need the proof.
Agree outcome metrics before the engagement begins. Specific. Measurable. Documented in the contract. So there is no ambiguity when you come to write the case study.
Build the case study process into the contract itself. Not as an afterthought. As a deliverable that gets created jointly during the engagement.
Secure the reference commitment as part of the commercial agreement, at the moment goodwill is at its highest. Specific language about reference calls, named testimonials, and case study publication rights.
Most founders treat first clients as revenue. The best founders treat them as infrastructure and the foundation every subsequent deal compounds on.
Case study. A healthtech founder I advised was about to sign a first contract at £120k with a major employer. The original contract had no reference clause, no agreed outcome metrics, and no case study process. We rewrote the contract before signing. Twelve months later, that case study had supported the next four contracts, combined value £840k, without requiring the founder to be in any of the initial sales conversations.
The first contract is infrastructure, not revenue. Price it to close. Design the case study in. Lock the reference commitment at signing.
If you have read this far, the framework will be sitting in your head as five labels - V, I, T, A, L. The next step is to find out which stage is actually your current commercial constraint.
Run this on yourself in five minutes. Score each statement 1–5, where 1 = strongly disagree, 5 = strongly agree.
1. VALIDATE. Our commercial evidence is translated into the specific language each buyer type can defend internally, not just clinical outcomes presented to commercial audiences.
2. IDENTIFY. We can name our top thirty target buyers by specific job title, organisation, current trigger event, and budget owner, not just our market category.
3. TARGET. We are focused on one primary go-to-market channel and have not opened a second channel until the first produced a referenceable case study.
4. ARTICULATE. Our commercial deck answers, before slide ten, why now, why us, and why we can deliver in the buyer's language.
5. LAND. Our first commercial contract was designed to produce a reference case study, with outcome metrics agreed upfront and reference commitments locked at signing.
If your total is below 15, the framework is your current commercial roadmap.
If your total is 15–22, you have momentum in two or three stages and a structural gap in the others - the £3,500 Diagnostic Sprint will tell you which gap to close first.
If your total is above 22, you have a working commercial system. The work now is compounding it, and the HealthTech Scale Playbook (six levers including financial scalability, team-and-culture, and ethical edge) is the next layer up.
Two next steps if this resonated
Download the HealthTech Scale Playbook. The six-lever playbook that sits underneath VITAL - Product-Market Integrity, Market Readiness, Compliance as Competitive Advantage, Financial Scalability, Team & Culture, The Ethical Edge. Free, immediately available, no gating beyond an email. Download here.
Book the £3,500 Diagnostic. A structured 90-minute session plus written report that maps your specific commercial position against VITAL and the six-lever playbook. The Diagnostic is the entry point to all Well Purposed advisory work, including the Q3 cohort that opens on Monday 8 June. Book the Diagnostic.
If you want to walk through your specific commercial position - reply to this email, DM me on LinkedIn, or book the Diagnostic directly.
The framework is now in your hands. The work is what you do with it.
- Sara
Founder, Well Purposed
LinkedIn 2026 Top Voice - HealthTech
P.S. The chapter of The Prevention Economy that develops this framework into book form (chapter 4: commercial architecture) is currently with literary agents. If you know an agent or publisher genuinely committed to prevention, public health, or the structural economics of healthcare, an introduction would be welcome.





Responses